Run tuyến giáp (Thyroid tremor)



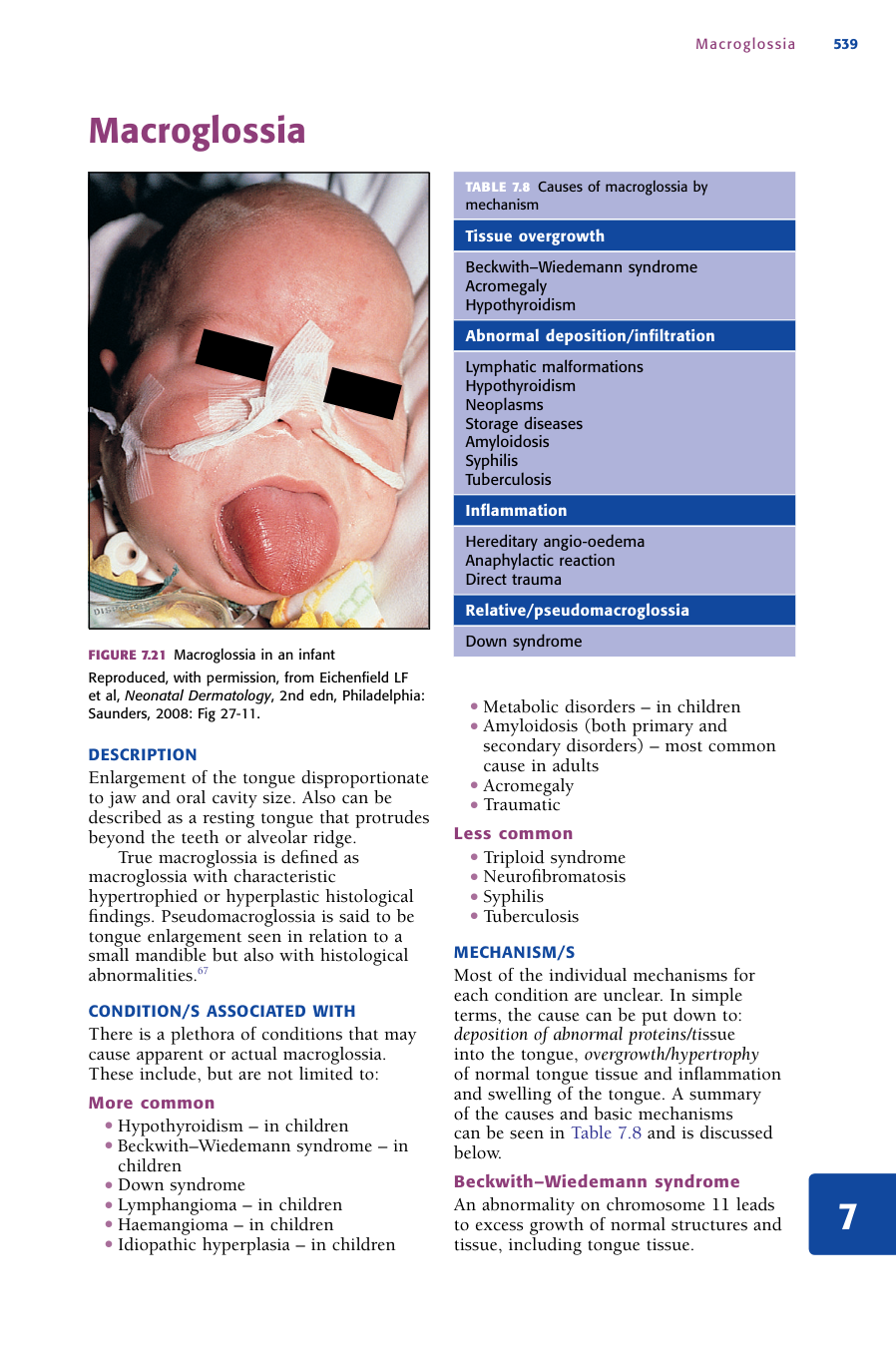














Mô tả: A high-tần số, low-amplitude run seen in the hands, face and head that worsens on movement. It is quite fine in appearance and supra-sinh lý. Delayed or slower-than-bình thường reflexes, đặc biệt a slow relaxation giai đoạn of the reflex. Abnormally low máu pressure, thường dưới 100 mmHg systolic. Enlargement of the tongue disproportionate to jaw and oral khoang size. Also có thể described as a resting tongue that protrudes beyond the teeth or alveolar ridge. True macroglossia được định nghĩa là macroglossia with đặc điểm hypertrophied or hyperplastic histological phát hiện. Pseudomacroglossia is said to be tongue enlargement seen in relation to a small mandible but also with histological abnormalities.67 One or more sharply demarcated yellow- brown plaques on the anterior pretibial region. Separation of the nail plate from the nail bed. The development of facial flushing, neck distension, engorged neck veins, stridor and raised JVP when a bệnh nhân raises and holds the arms above the head. Periodic liệt presents as episodes of painless cơ yếu that are thường sudden and liên quan đến preserved consciousness. Proximal cơ are affected hơn distal cơ, and reflexes are decreased or absent. Periodic liệt liên quan đến hypokalaemia. An excess of máu in a part or, by extension, a red florid complexion.37 Although strictly more a triệu chứng than a sign, excessive drinking có thể witnessed and is thường linked to polyuria. Polydipsia is the mạn tính excessive sensation of thirst and intake of fluid.37 Differentiation nên made between true thirst do dehydration-causing polyuria and that do a dry mouth alone (do effects of drugs or local factors). Passing of a large volume of urine within a defined thời kỳ of time.37 Although not truly a sign, it has value in a number of endocrinological and thận tình trạng, and in some settings có thể measured. Thickening of the da limited to the pre-tibial area. tuy nhiên, as the thickening có thể occur in other areas, the term ‘tuyến giáp dermopathy’ is more correct. bất thường protrusion of one or both jaws, đặc biệt the mandible, relative to the broader facial skeleton.37 yếu of the proximal cơ of the girdle bao gồm the quadriceps and biceps. có thể easily demonstrated by asking the bệnh nhân to rise from a seat andor to pretend to be brushing their hair or hanging washing on the clothes line. Pedunculated papules or nodules that are thường located on the eyelids, neck and axillae.90 Steroid acne differs from bình thường acne vulgaris in that it is of uniform size and đối xứng phân bố and is thường present on the neck, chest and back. It is thường flesh or pink-to-red coloured, with dome-shaped papules and pustules.
Nguyên nhân: • cường giáp • suy giáp • Multiple neurological tình trạng (xem Chapter 5, ‘Neurological signs’) • Anorexia nervosa • tiến triển age • Drugs (đặc biệt beta-blockers) • Hypothermia • Addison’s bệnh • suy giáp There is a plethora of tình trạng that có thể gây ra apparent or actual macroglossia. These bao gồm, but are not limited to: Thường gặp • suy giáp – in children • Beckwith–Wiedemann hội chứng – in children • Down hội chứng • Lymphangioma – in children • Haemangioma – in children • vô căn tăng sản – in children • Metabolic rối loạn – in children • Amyloidosis (both nguyên phát and thứ phát rối loạn) – most thường gặp cause in adults • to đầu chi • Traumatic Ít gặp • Triploid hội chứng • Neurofibromatosis • Syphilis • Tuberculosis • đái tháo đường Thường gặp • Trauma • nhiễm trùng • Psoriasis Ít gặp • cường giáp • Sarcoidosis • Connective mô rối loạn • Retrosternalsubsternal goitre – thường gặp • khối u • cường giáp • Congenital – most forms Thường gặp • mạn tính alcoholism • Cushing’s bệnh • Parenchymal phổi bệnh • Menopause Ít gặp • Polycythaemia • Hypernephroma • SVC obstruction • Mitral hẹp • Carcinoid hội chứng Thường gặp • đái tháo đường mellitus • đái tháo đường insipidus • Anticholinergics Ít gặp • Hypercalcaemia • Psychogenic polydipsia • Sjögren’s hội chứng • nguyên phát hyperaldosteronism Thường gặp • đái tháo đường mellitus • đái tháo đường insipidus • Excess IV fluids • Osmotic mannitol infusion, radiocontrast media, high-protein tube feeds • Drugs (e.g. diuretics, lithium, caffeine) • Post obstructive diuresis Ít gặp • Hypokalaemia • Hypercalcaemia • Psychogenic polydipsia (e.g. schizophrenia) • Excess IV fluids • Cushing’s hội chứng • nguyên phát hyperaldosteronism • Inability to concentrate urine: sickle tế bào trait or bệnh, mạn tính pyelonephritis, amyloidosis • Graves’ bệnh • Congenital defects • to đầu chi Many potential causes bao gồm, but not limited to: Thường gặp • cường giáp • suy giáp • Cushing’s hội chứng • Peripheral bệnh thần kinh • Polymyalgia rheumatica Ít gặp • Hyperparathyroidism • Sarcoidosis • Coeliac bệnh • Polymyositis • Dermatomyositis • di truyền cơ dystrophies • bình thường variant • đái tháo đường • to đầu chi Thường gặp • Endogenous and exogenous androgen sources • đái tháo đường • Drug liệu pháp Ít gặp • Hodgkin’s bệnh • HIV nhiễm trùng
Cơ chế: The run được cho là be a result of increased sympathetic activity do excess tuyến giáp hormone inducing a boost in beta-adrenergic sensitivity and activity.58 In suy giáp, giảm phản xạ được cho là be related to decreased cơ levels of myosin ATPase, causing a delay in cơ contraction60 and a slowing in the tỷ lệ of calcium re-accumulation in the sarcoplasmic endoplasmic reticulum,61 which is needed for bình thường cơ contraction and relaxation. Numerous causes, xem Chapter 3, ‘Cardiovascular signs’. Addison’s bệnh Dehydration and volume loss is the nguyên phát cause of hypotension in Addison’s bệnh. Mineralocorticoids regulate sodium retention and potassium excretion in the urine, sweat, saliva and GI tract. A deficiency of mineralocorticoids and, to a much lesser extent, corticosteroids dẫn đến salt teo and failure to concentrate urine, thus producing decreased circulatory volume, dehydration and hypotension. Deficiency of glucocorticoids (adrenaline) có thể also lower the basal tone of the vasculature and, hence, resting systolic máu pressure. Most of the individual cơ chế for each tình trạng are unclear. In simple terms, the cause có thể put down to: deposition of bất thường proteinstissue into the tongue, overgrowthhypertrophy of bình thường tongue mô and viêm and swelling of the tongue. A summary of the causes and basic cơ chế có thể seen in Bảng 7.8 and is discussed below. Beckwith–Wiedemann hội chứng An abnormality on nhiễm sắc thể 11 dẫn đến excess growth of bình thường cấu trúc and mô, bao gồm tongue mô. Bảng 7.8 nguyên nhân của macroglossia by mô overgrowth Beckwith–Wiedemann hội chứng to đầu chi suy giáp bất thường depositioninfiltration Lymphatic malformations suy giáp Neoplasms Storage bệnh Amyloidosis Syphilis Tuberculosis viêm di truyền angio-phù Anaphylactic reaction Direct trauma Relativepseudomacroglossia Down hội chứng Macroglossia 540 suy giáp được cho là be as a result of myocyte phì đại and deposition of myxphù, which dẫn đến accumulation of fluid.68,69 Amyloidosis In nguyên phát or thứ phát amyloidosis, there is excess production of an bất thường protein (amyloid). This protein có thể deposited in the tongue mô, leading to macroglossia. to đầu chi to đầu chi is a rối loạn of excess growth hormone, which stimulates a further excess of insulin growth factor. It is thought that these growth factors stimulate phì đại of various mô, bao gồm the tongue, leading to phì đại and macroglossia. Lymphangioma Lymphangioma is a malformation and tăng sản of the lymphatic hệ thống. When this occurs near or dẫn đến deposition into the tongue mô, macroglossia có thể ensue. The cơ chế has not been elicited. It is known that NLD is a mạn tính granulomatous viêm rối loạn, with connective mô thoái hóa; tuy nhiên, its link to glucose level and cơ chế has not been established.70 Theories bao gồm: • a form of miễn dịch-mediated vasculitis • bất thường collagen deposition • microangiopathy • impaired neutrophil migration. The cơ chế, aside from trauma, is unclear. When the arms are raised, the ring of the ngực inlet is brought upwards and gets stuck on the goitre. The goitre is said to ‘cork’ the ngực inlet and, in doing so, compresses the adjacent internal jugular veins. máu backs up, causing distension of the neck veins and facial plethora. Stridor occurs with pressure on the upper airway from any mass, be it khối u or goitre. Defects in cơ ion channels are the key cause of thyrotoxic periodic liệt, although the how or why is unclear.72 cường giáp increases the activity of the Na+K+ pumps on cơ tế bào, producing a large and rapid shift of potassium intracellularly and leading to hyperpolarisation and absent cơ tế bào depolarisation. Plethora có thể gây ra bởi an increased volume of máu flow to the face, any factor that có thể dilate the máu mạch in the area or máu mạch being closer to the da’s surface. Cushing’s bệnh In Cushing’s bệnh excess cortisol causes degradation and teo of the epidermis and underlying connective mô. This dẫn đến apparent thinning of the da and the appearance of facial plethora.2 Carcinoid hội chứng Excess serotonin release seen in carcinoid hội chứng causes the giãn of da mạch and the appearance of plethora. Mitral hẹp Mitral hẹp dẫn đến increased pressure from the left side of the tim. This dẫn đến increased venule and tĩnh mạch pressure, engorging small capillaries and causing plethora. Parenchymal phổi bệnh Parenchymal phổi bệnh có thể gây ra raised phổi artery pressure and, do đó, pressure back to the right side of the tim and into the tĩnh mạch hệ thống. This, in turn, can increase tĩnh mạch pressure, causing engorgement of máu mạch in the face. thường thứ phát to polyuria and as a response to dehydration (from đái tháo đường mellitus, đái tháo đường insipidus, hypercalcaemia). Xem ‘Polyuria’ in this chapter. Sjögren’s hội chứng In Sjögren’s hội chứng, an tự miễn rối loạn stops the production of saliva (and affects lacrimal glands). The result of this is a dry mouth, and the bệnh nhân continues to drink in order to alleviate the discomfort. Psychogenic polydipsia This được cho là be a multi-factorial malfunction of the hypothalamic thirst centre, involving the mạn tính intake of excessive amounts of water, which reset the thirst and ADH cue points. In other words, bệnh nhân need to drink more to satisfy their feeling of thirst andor ADH is inappropriately suppressed. Positive triệu chứng of schizophrenia, compulsive behaviour, stress reactions, drinking to counteract anti-cholinergic side effects to thuốc and elevated dopamine responses stimulating the thirst centre have all been suggested as possible triggers. nguyên phát hyperaldosteronism Excess aldosterone dẫn đến hypokalaemia, which, in turn, causes a decrease in aquaporin water tubules in the cortical collecting duct. With less water able to be reabsorbed, obviously more is excreted, leading to polyuria. Polyuria 547 Polyuria Polyuria thường develops from two key free water. 1 In some tình trạng, there is a high ‘osmotic load’ of the serum being filtered through the thận do the excretion of non-absorbable solutes (e.g. glucose). This dẫn đến an osmotic diuresis. Put simply, this means large quantities of bigger solutes in the thận tubules of the thận hold water ‘in’, rather than allowing it to be reabsorbed. ngoài ra, the concentration gradient in the proximal tubules is altered, affecting sodium reabsorption and urine concentration. 2 The second main cơ chế is an inappropriate excretion of free water,74 which is thường do abnormalities in vasopressin production or in response to vasopressin plus an inability to concentrate urine. đái tháo đường mellitus Polyuria in đái tháo đường mellitus is do osmotic diuresis from excretion of excess glucose. Water is drawn out by osmosis do the high filtration of glucose in the thận. Polyuria in this setting indicates symptomatic tăng đường huyết. đái tháo đường insipidus đái tháo đường insipidus (DI) có thể further broken down into central and peripheral loại. Nephrogenic DI có thể further classified as either congenital or acquired. The basic cơ chế are shown in Bảng 7.9. Post obstructive diuresis Seen when hai bên urinary tract obstruction is relieved and được cho là be do: 1 the excretion of retained urea, causing an osmotic diuresis 2 obstruction of ureters raising pressure in the tubules of the thận and impairing sodium chloride reabsorption. With less sodium being reabsorbed, concentration gradients in the thận are not maintained and water is lost with sodium chloride. Lithium Lithium has a number of effects on the thận. Its cơ chế in causing polyuria is hypothesised to be by impairing the stimulatory effect of ADH on adenylate cyclase75 that, when present, normally dẫn đến the production of water channels in the cortical collecting duct. Other effects lithium có thể have bao gồm: • partially inhibiting the ability of aldosterone to increase ENAC expression and salt reabsorption; as a consequence, salt is lost in the urine and water follows it out76 • potentially inhibiting sodium reabsorption in the cortical collecting channel; decreased sodium reabsorption dẫn đến salt teo and water follows the sodium out in the urine.77 Polyuria 548 Bảng 7.9 cơ chế of đái tháo đường insipidus (DI) Abnormality C E N T R A L D I vô căn or thứ phát to any rối loạn that dẫn đến damage to the vasopressin (ADH)-secreting nơron in the posterior pituitary Inadequate excretion of ADH from the pituitary → inadequate activation of the V2 thụ thể and aquaporins → water is not reabsorbed and is lost in urine C O N G E N I TA L N E P H R O G E N I C D I đột biến of V2 thụ thể on distal tubule of the thận V2 thụ thể is not responsive to ADH stimulation → failed activation of aquaporin channels → water not appropriately retained and so lost in urine đột biến of aquaporin water channel đột biến of aquaporin water channel does not allow for adequate reuptake of water when the V2 thụ thể is stimulated by ADH. The water is excreted in urine A C Q U I R E D N E P H R O G E N I C D I Hypokalaemia Hypokalaemia dẫn đến decreased expression of aquaporin 2 channels → decreased water uptake and do đó increased diuresis Hypercalcaemia Hypercalcaemia dẫn đến decreased expression of aquaporin 2 channels → decreased water uptake and do đó increased diuresis Polyuria: Cushing’s hội chứng 549 Polyuria: Cushing’s hội chứng Excess glucocorticoids have been shown to inhibit osmosis-stimulated ADH secretion as well as directly enhancing free water clearance,37 thus producing polyuria. tăng đường huyết causing osmotic diuresis is hiếm khi the cause of polyuria in Cushing’s hội chứng. PSYCHOGENIC POLYURIA cơ chế Seen in concert with psychogenic polydipsia; xem ‘Psychogenic polydipsia chapter. Pre-tibial myxoedema (tuyến giáp dermopathy) 550 Pre-tibial myxoedema (tuyến giáp dermopathy) The cơ chế behind pre-tibial myxoedema is similar to (or an extension of) that seen in Graves’ ophthalmopathy. Immunological, tế bào and mechanical factors contribute to the production and localisation of glycoaminoglycans and the sequestration of fluid to produce the đặc điểm da changes. In Graves’ bệnh, lymphocytes infiltrate the dermal mô around the pre-tibia.78 It is also hypothesised that in Graves’ bệnh there is an hơn-expression of TSH thụ thể at certain sites, bao gồm the pre-tibial area. These thụ thể are stimulated by kháng thể produced by local miễn dịch tế bào, which dẫn đến fibroblast secretion of glycoaminoglycans and the sequestration of fluid. Mechanical forces play a role in the localisation of the da changes.79–81 Dependent phù, produced by reduced lymphatic return, increases the pooling of bệnh-related cytokines and chemokines and other factors that increase the effect82 in the immediate area, producing the đặc điểm da changes. The final cơ chế of prognathism in to đầu chi is complex and unclear. It is related to the excess production of growth hormone and insulin-like growth factor-1, causing excess xương growth in the jaw. In to đầu chi, there is an excess production of growth hormone (GH) from the anterior pituitary gland. GH has effects on body mô both directly and indirectly through the stimulation of insulin-like growth factor-1 (IGF-1). Both IGF-1 and GH affect chondrocytes and có thể gây ra excess production. Disproportionate growth of the mandible stimulated by a surplus of GH and IGF-1 có thể contribute to prognathism in bệnh nhân with to đầu chi. Hyperthyroid The cơ chế is unclear. Possible contributing factors bao gồm:84–87 • increased tế bào metabolism and energy utilisation • increased catabolism and protein degradation • inefficient energy utilisation • disturbance of the chức năng of cơ fibres do increased mitochondrial respiration • accelerated protein degradation and lipid oxidation • enhanced beta-adrenergic sensitivity. suy giáp Lack of tuyến giáp hormone slows bình thường metabolic chức năng, bao gồm protein turnover-impaired carbohydrate metabolism.88,89 As a consequence, cơ tế bào do not have nor utilise energy as efficiently, resulting in yếu. Hyperparathyroidism The cơ chế is unclear. It is known that PTH does impact on skeletal cơ but, given that the variables it affects bao gồm calcium, phosphate and vitamin D, it is difficult to pinpoint the exact cause of the proximal cơ yếu.83 Cushing’s hội chứng The catabolic effects of glucocorticoids break down proteins in the cơ fibres, causing yếu. Additional factors bao gồm hypokalaemia and physical inactivity. In some cases hypokalaemia, gây ra bởi excess mineralocorticoids causing potassium excretion via the thận, có thể exacerbate the situation. This gây ra bởi an imbalance in the electrochemical gradient between the intracellular and extracellular spaces. Simply put, a gradient of potassium is required between the two spaces, in order for tế bào to effectively ‘fire’ – i.e. depolarise and repolarise. Decreasing the potassium outside a tế bào causes hyper-polarisation of the tế bào, making it harder for the tế bào (in this case proximal skeletal cơ fibres) to fire. Physical inactivity of bệnh nhân with Cushing’s hội chứng also plays a role. The cơ chế is unclear. Theories have included: • frequent irritation • bình thường ageing process • hormone levels (e.g. high levels of growth hormone in to đầu chi). Steroid excess in Cushing’s hội chứng có thể exacerbate existing acne; tuy nhiên, it có thể more thường be an acne-like tình trạng called malassezia (pityrosporum) folliculitis.94 This đặc trưng bởi an alteration in bình thường da tình trạng, bao gồm changes to miễn dịch, sebum production and the growth of bình thường da flora.95 The end result is plugging of the hair follicle and an environment that allows a particular yeast (Malassezia furfur) to proliferate. In Cushing’s bệnh, it is possible that alterations of miễn dịch gây ra bởi corticosteroid excess will allow nấm proliferation. High levels of androgens and sebum production có thể also contribute.
Ý nghĩa lâm sàng: It is seen in lên đến 69–76%41,59 of bệnh nhân with cường giáp with a specificity of 94%41 and PLR of 11.4. If present in a bệnh nhân with suspected cường giáp, it is a valuable sign. Hyporeflexiadelayed ankle jerks (Woltman’s sign) 537 Hyporeflexiadelayed ankle jerks (Woltman’s sign) There are mixed reports on the value of the reflex (đặc biệt Achilles reflex) as a chẩn đoán sign for suy giáp and for cường giáp. The half-relaxation time in well people is khoảng 240 to 320 ms.62 • One study found 75% of hypothyroid bệnh nhân had a delayed relaxation giai đoạn, with a PPV of 72. • Another study found 91% of bệnh nhân with cường giáp and 100% of hypothyroid bệnh nhân had a half- relaxation time outside the bình thường range, suggesting a very high sensitivity of the test.63 • Other studies64 found lên đến 35% of hyperthyroid and 12% of hypothyroid bệnh nhân were in the bình thường range. All of these studies were completed using specialised recording devices that would not be routinely used in day-to-day practice. hơn nữa, having readily available tuyến giáp chức năng tests makes this test less applicable in today’s practice in isolation from other signs or triệu chứng. Hypotension 538 Hypotension A thường gặp sign in cấp tính nguyên phát adrenal insufficiency – lên đến 88% of bệnh nhân exhibit hypotension.2 tuy nhiên, given the myriad nguyên nhân của hypotension, its value as an isolated sign is limited. Conversely, the presence of hypertension is a strong negative predictor of a chẩn đoán of Addison’s bệnh.65,66 Macroglossia 539 Macroglossia There are few evidence-based reviews on the value of macroglossia as a sign. tuy nhiên, if it is seen, it will almost luôn be bệnh lý and investigation as to the cause is needed. Necrobiosis lipoidica diabeticorum (NLD) 541 Necrobiosis lipoidica diabeticorum (NLD) One older study showed a strong association with tự miễn (loại 1) đái tháo đường, whereby almost two-thirds of bệnh nhân with lesions had đái tháo đường and 5–10% had glucose tolerance abnormalities.71 A more recent study showed only 11% of bệnh nhân with NLD had đái tháo đường,16 and the tỷ lệ hiện mắc of NLD in bệnh nhân with đái tháo đường was only 0.3–3.0%.71 Onycholysis (Plummer’s nail) 542 Onycholysis (Plummer’s nail) There is little evidence of the tỷ lệ hiện mắc of onycholysis in hyperthyroid bệnh nhân. Other signs and triệu chứng are likely to present themselves trước khi onycholysis. Pemberton’s sign 543 Pemberton’s sign Goitre ngực inlet ( ‘neck of bottle’ ) Internal jugular veins Too small to obstruct ngực inlet Elevating arms pulls ngực inlet ( ‘neck of bottle’ ) up into goitre ( ‘cork’ ) bình thường tuyến giáp: Substernal goitre: The tần số of Pemberton’s sign chưa được biết rõ in bệnh nhân with substernal goitres.23 Periodic liệt 544 Periodic liệt Increased T4 Raised adrenergic response Hypokalaemia Intracellular shift of potassium Increased Na+K+-ATPase activity Increased insulin resistance Disrupted ion channels Hyperpolarisation Periodic liệt It is a hiếm gặp event affecting between 2% and 20%, and 0.1% and 0.2%, in Asian and American populations, respectively. There is no correlation between mức độ nặng of cường giáp and the manifestation of liệt.73 Plethora 545 Plethora Seen in 70% of bệnh nhân with Cushing’s hội chứng,2 plethora has only limited specificity given its many possible aetiologies. Polydipsia 546 Polydipsia Pre-tibial myxoedema is a hiếm gặp sign clinically and is almost luôn preceded by the Thường gặp eye signs of Graves’ bệnh. It is seen in 0.5% to 4.3% of bệnh nhân with a history of thyrotoxicosis and in lên đến 13% of bệnh nhân with Graves’ ophthalmopathy,78,83 Interestingly, forearm changes of so-called pre-tibial myxoedema are thường present in cases of clinically definite Graves’ bệnh, and có thể detected by ultrasound as da thickening. Prognathism 551 Prognathism Prognathism virtually không bao giờ occurs in to đầu chi in isolation, so its value as a chẩn đoán sign is limited. Conversely, if no other signs liên quan đến to đầu chi are present, congenital abnormality is the most likely cause. Proximal bệnh cơ 552 Proximal bệnh cơ Seen in 60–80% of bệnh nhân with cường giáp, but also seen in numerous other endocrinological and other rối loạn. It is not thường gặp for proximal bệnh cơ to be an initial presentation of cường giáp. In suy giáp, it is seen in 30–80% of bệnh nhân and, do đó, has only trung bình sensitivity and low specificity. da tags (acrochordon) 553 da tags (acrochordon) Of limited value, as da tags are very thường gặp in the general population. It has been claimed the tỷ lệ mới mắc is greater in đái tháo đường, obese bệnh nhân as well as those with to đầu chi. Interestingly, tuy nhiên, recent studies have shown an association between the presence of da tags and insulin resistance.91,92 ngoài ra, a small study has suggested that da tags are increased in bệnh nhân with metabolic derangements and có thể present as a nguy cơ marker of cardiovascular bệnh and atherosclerosis.93 Steroid acne 554 Steroid acne