Bệnh võng mạc đái tháo đường (Diabetic retinopathy)










Mô tả: đái tháo đường retinopathy is an umbrella term được sử dụng để describe a number of đặc điểm changes seen in the eye in the setting of đái tháo đường. Some of the terms and causes overlap with hypertensive retinopathy and have thường gặp final con đường. Xem ‘Hypertensive retinopathy’ in Chapter 3, ‘Cardiovascular signs’. Broadly speaking, đái tháo đường retinopathy có thể broken down into the thể shown in Bảng 7.1. An unusual prominence of the trán. Lactation that occurs in the absence of breastfeeding in females. It is luôn bệnh lý in males. An enlargement of the tuyến giáp gland causing a swelling in the front of the neck,37 which is thường both visible and palpable on thăm khám. Characterised by a ring of small, firm flesh-coloured or red papules, thường found on the dorsal surfaces of hands and feet.44 They có thể develop a rolled border with central clearing. có thể là localised or disseminated across the body, subcutaneous or perforating (reaching deeper into subcutaneous mô). Graves’ ophthalmopathy encompasses a number of eye signs and changes thường xuyên seen in Graves’ bệnh. The tiến triển in mức độ nặng of these is classified in Bảng 7.5. and thường the underlying cơ chế contribute to the development of multiple signs. Bảng 7.6 summarises a collection of signs that có thể là seen on physical exam. Graves’ ophthalmopathy (orbitopathy) 527 Cross-reacts with TSH thụ thể on effector tế bào (fibroblasts, adipocytes etc.) Autoantibody against TSH thụ thể (TSHR) Graves ophthalmopathy insulin-like factor stimulated Subgroup of fibroblasts differentiate into adipocytes Fibroblasts stimulated to produce hyaluronan Infiltrated CD4, CD8 and B tế bào release cytokines (IL-1, TFN and proadipogenic substances) Fluid retention and swelling xơ of extraocular cơ Increased intra-orbital pressure tĩnh mạch congestion viêm tế bào infiltrate to orbital cơ, glands and interstitium
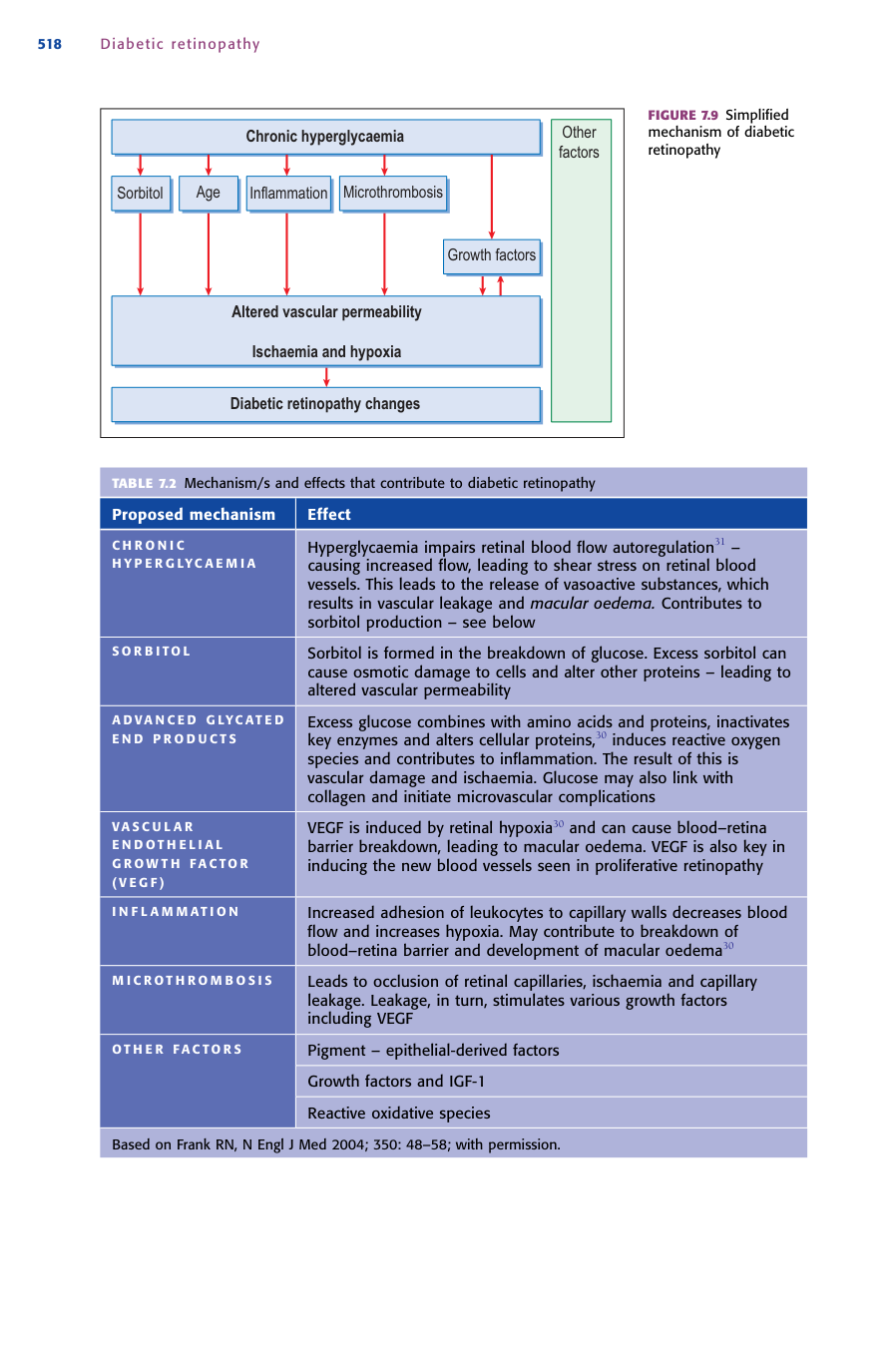
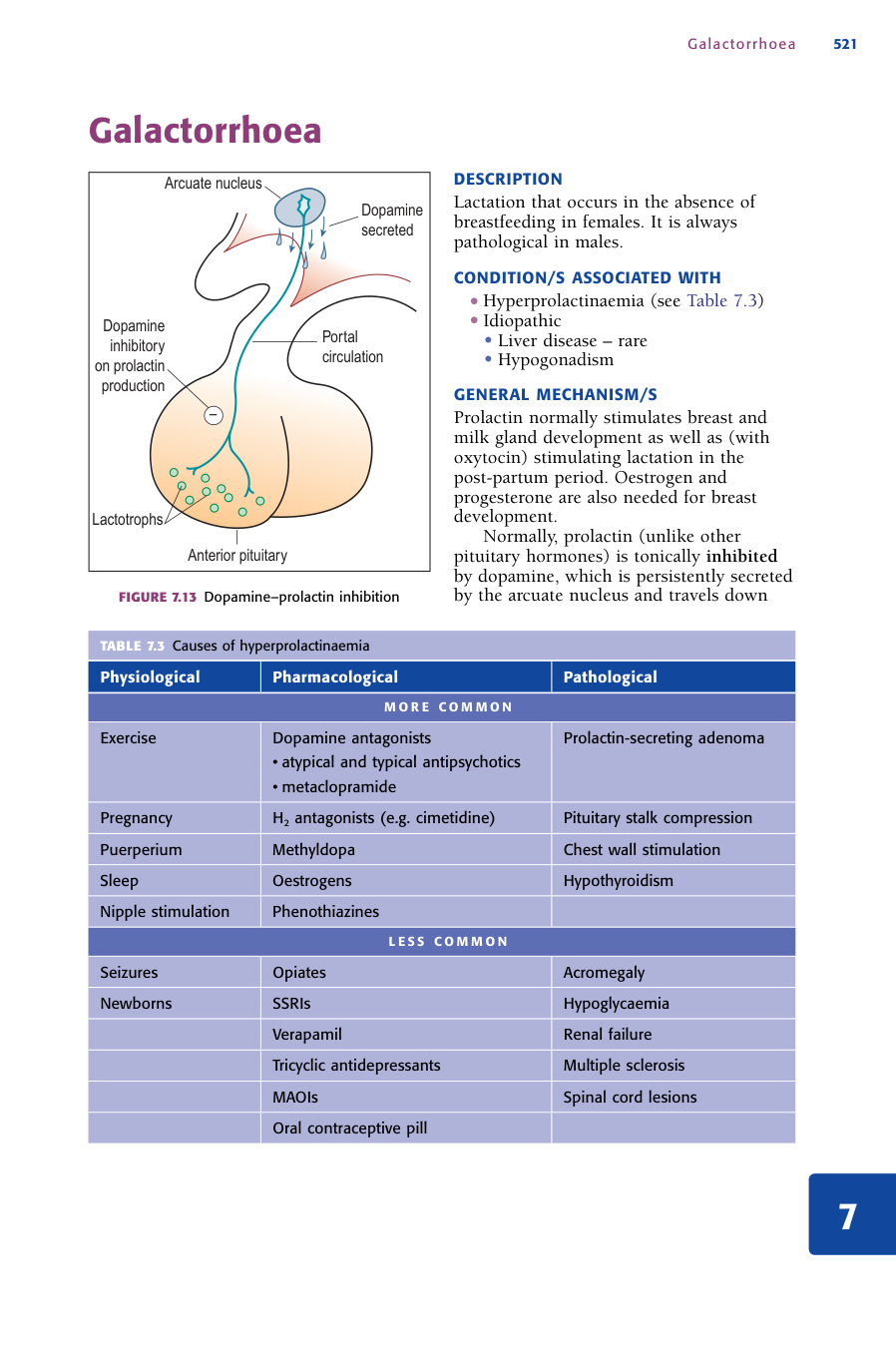
Nguyên nhân: • đái tháo đường • Hypertensive retinopathy can also display similar changes and macular phù có thể được điều trị with success in most cases to prevent blindness, both screening for and detecting the lâm sàng sign in any setting is essential. Changes liên quan đến đái tháo đường retinopathy are seen in: • almost all bệnh nhân who have had loại 1 đái tháo đường for 20 years • 80% of bệnh nhân who have had loại 2 đái tháo đường for 20 years. sau 10 years, proliferative retinopathy is seen in 50% of bệnh nhân with loại 1 diabetes33 and 10% of bệnh nhân with loại 2 đái tháo đường.32 đái tháo đường retinopathy 518 Other factors Altered mạch máu permeability thiếu máu cục bộ and hypoxia mạn tính tăng đường huyết Sorbitol Age viêm Microthrombosis Growth factors đái tháo đường retinopathy changes Thường gặp • to đầu chi – thường associated but to đầu chi itself is a hiếm gặp hormonal • Fragile X hội chứng – a thường gặp cause of mental retardation in males, liên quan đến a large hộp sọ bao gồm prominent trán • Extramedullary haematopoiesis – xem the mô tả under ‘Chipmunk facies’ in Chapter 4, ‘Haematological oncological signs’ Galactorrhoea 521 Galactorrhoea Dopamine inhibitory on prolactin production Anterior pituitary Lactotrophs Arcuate nucleus Dopamine secreted Portal circulation • Hyperprolactinaemia (xem Bảng 7.3) • vô căn • gan bệnh – hiếm gặp • Hypogonadism • Graves’ bệnh • Hashimoto’s bệnh • Congenital • Adenomatous (tuyến giáp adenoma) • Iodine deficiency • Toxic multinodular • tuyến giáp ung thư biểu mô Thường gặp • nhiễm trùng and immunisations (e.g. herpes zoster; hepatitis B, C) • Trauma • đái tháo đường mellitus (historically, loại 1 DM) Ít gặp • Drugs (e.g. gold liệu pháp, allopurinol, amlodipine) • ác tính (e.g. Hodgkin’s and non-Hodgkin’s lymphoma, leukaemia) • Rheumatoid arthritis • Graves’ bệnh
Cơ chế: The cơ chế behind the changes seen in đái tháo đường retinopathy is very complex and as yet has not been fully explained. mạn tính tăng đường huyết được cho là be the main factor leading to đái tháo đường retinopathy,30 by commencing a series of changes that ultimately dẫn đến two key bệnh lý states: 1 altered mạch máu permeability – disrupted or leaky mạch 2 thiếu máu cục bộ of the võng mạc with associated neovascularisation. These changes are implicated in the vision-threatening forms of macular đái tháo đường retinopathy Bảng 7.1 đái tháo đường retinopathy changes Nonproliferative retinopathy Cotton wool spots thiếu máu cục bộ swelling of the thị giác dây thần kinh layer causes a white, round or patchy appearance Dot and blot haemorrhages Larger red dots with distinct (dot) or indistinct (blot) borders Hard exudates Lipids deposited within the võng mạc create white or yellowish deposits with a waxy appearance Microaneurysms Distinct round red dots Proliferative retinopathy Neovascularisation arising from the thị giác disc or mạch Macular phù Thickening and phù involving the macula (có thể occur at any giai đoạn of proliferative or non-proliferative đái tháo đường retinopathy) phù and proliferative đái tháo đường retinopathy. Of course, there are many additional bệnh lý processes that also contribute to the development of these two states. Bảng 7.2 contains some of the key components. retinopathy Bảng 7.2 cơ chế and effects that contribute to đái tháo đường retinopathy Proposed cơ chế Effect C H R O N I C H Y P E R G LYC A E M I A tăng đường huyết impairs võng mạc máu flow autoregulation31 – causing increased flow, leading to shear stress on võng mạc máu mạch. This dẫn đến the release of vasoactive substances, which dẫn đến mạch máu leakage and macular phù. Contributes to sorbitol production – xem below S O R B I TO L Sorbitol is formed in the breakdown of glucose. Excess sorbitol có thể gây ra osmotic damage to tế bào and alter other proteins – leading to altered mạch máu permeability A D VA N C E D G LYC AT E D E N D P R O D U C T S Excess glucose combines with amino acids and proteins, inactivates key enzymes and alters tế bào proteins,30 induces reactive oxygen species and contributes to viêm. The result of this is mạch máu damage and thiếu máu cục bộ. Glucose có thể also link with collagen and initiate microvascular biến chứng VA S C U L A R E N D O T H E L I A L G R O W T H FA C TO R ( V E G F ) VEGF is induced by võng mạc hypoxia30 and có thể gây ra máu–võng mạc barrier breakdown, leading to macular phù. VEGF is also key in inducing the new máu mạch seen in proliferative retinopathy I N F L A M M AT I O N Increased adhesion of leukocytes to capillary walls decreases máu flow and increases hypoxia. có thể contribute to breakdown of máu–võng mạc barrier and development of macular oedema30 M I C R O T H R O M B O S I S dẫn đến occlusion of võng mạc capillaries, thiếu máu cục bộ and capillary leakage. Leakage, in turn, stimulates various growth factors bao gồm VEGF O T H E R FA C TO R S Pigment – epithelial-derived factors Growth factors and IGF-1 Reactive oxidative species Based on Frank RN, N Engl J Med 2004; 350: 48–58; with permission. đái tháo đường retinopathy 519 In to đầu chi, too much circulating growth hormone causes excess growth of the hộp sọ and, đặc biệt, the xương of the trán. Prolactin normally stimulates breast and milk gland development as well as (with oxytocin) stimulating lactation in the post-partum thời kỳ. Oestrogen and progesterone are also needed for breast development. Normally, prolactin (unlike other pituitary hormones) is tonically inhibited by dopamine, which is persistently secreted by the arcuate nucleus and travels down Bảng 7.3 nguyên nhân của hyperprolactinaemia sinh lý Pharmacological bệnh lý M O R E C O M M O N Exercise Dopamine antagonists • atypical and typical antipsychotics • metaclopramide Prolactin-secreting adenoma Pregnancy H2 antagonists (e.g. cimetidine) Pituitary stalk compression Puerperium Methyldopa Chest wall stimulation Sleep Oestrogens suy giáp Nipple stimulation Phenothiazines L E S S C O M M O N Seizures Opiates to đầu chi Newborns SSRIs hạ đường huyết Verapamil thận failure Tricyclic antidepressants Multiple sclerosis MAOIs tủy sống lesions Oral contraceptive pill Galactorrhoea 522 the pituitary stalk (on the tuberoinfundibular axis) and stops tế bào in the anterior pituitary (lactotrophs) from producing prolactin (xem Hình 7.13). do đó, hyperprolactinaemia and galactorrhoea có thể là gây ra bởi: 1 excess prolactin secretion 2 disruption of the bình thường inhibitory process of dopamine 3 failed excretion of prolactin. Note: Having hyperprolactinaemia does not necessarily mean galactorrhoea will follow. Selected drug cơ chế The predominant effect of thường used antipsychotics (e.g. olanzapine, risperidone) and anti-nausea thuốc (metaclopramide) is do blocking of dopamine. This có thể gây ra the inhibitory of effect of dopamine on prolactin to be reduced, thereby producing hyperprolactinaemia. Methyldopa depletes dopamine stores and competitively inhibits L-dopa conversion to dopamine, thereby reducing dopamine and do đó inhibition of prolactin. Verapamil has a side effect of directly stimulating lactotrophs,34 thus producing more prolactin. SSRIs increase the level of serotonin available, which has a stimulating effect on prolactin secretion. Prolactinomas Prolactinomas are a loại of pituitary adenoma, which is a tân sản growth of pituitary lactotroph mô. Prolactinomas secrete prolactin in large quantities and are not effectively inhibited by bình thường levels of dopamine. Pituitary stalk compression Stalk compression by any cause (e.g. craniopharyngioma, trauma, pituitary adenoma) disrupts or destroys the bình thường tuberoinfundibular con đường that allows dopamine to travel from the arcuate nucleus, via the portal circulation, to the lactotrophs to inhibit prolactin secretion. Hyperprolactinaemia results. suy giáp In suy giáp thyrotrophin- releasing hormone (TRH) is elevated in a compensatory response to low thyroxine. TRH is a potent prolactin- releasing factor. Chest wall stimulation Chest wall stimulation do any cause (e.g. breast phẫu thuật, mechanical trauma, herpes zoster) can produce a neurogenic reflex to stimulate the production of prolactin2 via the suppression of dopamine. It is thought that stimuli are passed via the intercostal dây thần kinh to the posterior column of the tủy sống, to the thân não and then the hypothalamus where dopamine secretion is reduced.34 to đầu chi Hyperprolactinaemia and galactorrhoea có thể result from: 1 mass effect of the pituitary adenoma causing stalk compression 2 excess growth hormone that has a stimulatory effect on prolactin 3 in very hiếm gặp cases, a pituitary adenoma có thể produce both growth hormone and prolactin. thận failure Decreased clearance of prolactin được cho là be the cơ chế. Newborn galactorrhoea High maternal oestrogen levels pass through the placenta, causing development of the foetal breast mô. The cơ chế of goitre development depends on the underlying cause. tuy nhiên, the final thường gặp con đường for most goitres will involve one or more of the sau: 1 nguyên phát TSH stimulation (or TSHR stimulation by an kháng thể in Graves’ bệnh) of tuyến giáp tế bào causing tế bào tăng sản 2 TSH stimulation of tuyến giáp tế bào causing tế bào tăng sản thứ phát to low levels of tuyến giáp hormone through problems with tuyến giáp hormone production or secretion 3 autonomous hyperfunction. Bảng 7.4 summarises the various nguyên nhân của goitres and the relevant Graves’ bệnh tuyến giáp thụ thể kháng thể stimulate TSH thụ thể on the tuyến giáp gland, causing tế bào tăng sản and tuyến giáp gland phì đại Infiltration of miễn dịch tế bào có thể also contribute to enlargement Toxic multinodular goitre Autonomous hyperfunction. Goitres can change from TSH-dependent tăng sản to autonomous hyperfunction. Oxygen reactive species and other processes có thể precipitate gen mutations, leading to mạn tính activation of the Gs andor other proteins, which causes mạn tính proliferation of tuyến giáp cells2,38 Single toxic adenoma Autonomous hyperfunction as described above Iodine deficiency In iodine deficiency, the cause of the goitre is still TSH hơn- stimulation and tế bào tăng sản but it is thứ phát to impaired hormone synthesis. An iodine level of dưới 0.01 mg (10 µg) per day impedes tuyến giáp hormone synthesis. In response to low levels of tuyến giáp hormones, more TSH is produced and secreted via feedback cơ chế, causing tế bào tăng sản Iodine excess Excess iodine can block the secretion of tuyến giáp hormones, leading to low levels and a compensatory rise in TSH, and do đó TSH-related tế bào hyperplasia39 Congenital rối loạn Defects in hormone synthesis dẫn đến a compensatory rise in TSH and, do đó, TSH-stimulated tế bào tăng sản Adenomatous Mutations in the TSH con đường, most thường the TSH thụ thể and Gs unit, dẫn đến excess cAMP and the production of a few ‘highly growth-prone tế bào’ that, when stimulated by TSH, grow exponentially hơn the homogenous surrounding mô, producing an adenoma40 Goitrogens (e.g. cabbage, turnips, lithium, sulfonylureas) Block secretion of tuyến giáp hormone39 Hypothyroid euthyroid goitres Hashimoto thyroiditis thứ phát rises in TSH and lymphocytic invasion are responsible for goitre formation in Hashimoto’s bệnh. In Hashimoto thyroiditis, lymphocytes are sensitised to the tuyến giáp gland and destroy bình thường architecture. This destruction in the gland causes a drop in T3 and T4, and a compensatory rise in TSH, which causes goitre development through tế bào tăng sản. Heavy lymphocytic infiltration also adds to the formation of the goitre Granuloma annulare 525 Granuloma annulare The cơ chế behind the development of connective mô surrounded by viêm infiltrate is not clear. 1 nguyên phát thoái hóa of connective mô initiating granulomatous viêm 2 lymphocyte-mediated miễn dịch reaction leading to macrocyte and cytokine activation and destruction of connective mô 3 a vasculitis or other microangiopathy causing mô injury. Much progress has been made towards identifying specific cơ chế in Graves’ bệnh. Key to the development of many of the signs is immunoreactivity against the thyrotropin thụ thể, bao gồm autoantibodies, and the dysregulation of bình thường orbital fibroblast chức năng by this tự miễn immunoreactivity.49 Through a variety of processes explained below, this dẫn đến mắt cơ swelling and xơ. In Graves’ bệnh anti-tuyến giáp thụ thể kháng thể are produced as part of the bệnh process. These kháng thể that act on the tuyến giáp also affect orbital fibroblasts. When stimulated by tuyến giáp autoantibodies and cytokines, fibroblasts proliferate and produce large amounts of hydrophilic hyaluronan, a loại of glycoaminoglycan that attracts and sequesters fluid. At the same time, a subgroup of fibroblasts differentiates into mature adipocytes. It is these two changes (with associated lymphocytic infiltration) that dẫn đến the enlarged mắt cơ and orbital fat pads seen in bệnh nhân with Graves’ ophthalmopathy. ngoài ra to this, stimulation of insulin-like growth factor thụ thể on orbital fibroblasts dẫn đến the recruitment of more activated T tế bào and miễn dịch tế bào. This further stimulates existing fibroblasts to produce prostaglandin E2 and hyaluronan,1 which accumulates between cơ fibres, making them bigger. Activated miễn dịch tế bào also produce proadipogenic substances that stimulate the maturation of more adipocytes, which expands mô volume even more. With the increase in size of soft mô and cơ involved with the orbit (do the combination of adipocytes, hylauronan and viêm tế bào infiltrates), pressure within the orbital khoang is increased – ultimately affecting the chức năng of the eye. It nên noted that, ngược lại to Graves’ ophthalmopathy, the eye sign of lid lag is a đặc điểm of tuyến giáp overactivity (cường giáp) do increased activity of the levator palpebrae superioris. Summary of eye sign cơ chế There are a large number of eye signs liên quan đến Graves’ bệnh. Some Upper lid retraction The upper eyelid is noticeably retracted, exposing an bất thường amount of the upper sclera. It có thể produce Dalrymple’s sign (described below) Contributing factors bao gồm:49 • Excess tuyến giáp hormone causes increased sympathetic stimulation of the superior tarsal cơ (aka Mueller’s cơ – a sympathetically innervated smooth cơ that assists in elevating the eyelid) • hơn-activation of the levator cơ as it contracts against a tight inferior rectus cơ • Scarring between levator and surrounding mô does not allow for bình thường closure Von Graefe’s sign A dynamic abnormality; as the eye moves down, the eyelid does not follow smoothly but at a slower tỷ lệ, exposing the superior limbus50 The specific cơ chế has not been elucidated. Likely a combination of factors contributing to upper lid retraction (xem above) Lagopthalmos Inability to close the eyes The specific cơ chế chưa được biết rõ. Likely a combination of factors contributing to upper lid retraction (xem above) Abadie’s sign Spasm of the levator palpebrae when retracting the upper eyelid The specific cơ chế chưa được biết rõ. Likely a combination of factors contributing to upper lid retraction (xem above) Dalrymple’s sign Widening of the palpebral fissure A combination of: 1) lồi mắt, making it more difficult for the eyelid to cover all of the eye; and 2) hypertonicityoveractivation of the levator and Mueller’s cơ, resulting in the upper lid retraction and hence widening of the palpebral fissure Retraction of the eyelids on outward stare so that the palpebral opening is abnormally wide Griffith’s sign Lower lid lag on upward gaze Most likely hơn-activitysympathetic stimulation of dây thần kinh supplying the lower eyelid, with or without mechanical restriction of cơ involved in eyelid closure Stellwag’s sign Infrequent and incomplete blinking, thường accompanied by Dalrymple’s sign bình thường blinking is mainly controlled by the obicularis oculi (closing the eye) and levator palpebrae (opening the eye) with Mueller’s cơ to assist in eye widening. Excess stimulation and hơn-activation of Mueller’s cơ and levator palpebrae do high levels of tuyến giáp hormone causes the opening element of blinking to be accentuated Graves’ ophthalmopathy (orbitopathy) 529 Name song thị ’Double vision’ viêm, swelling and cuối cùng xơ of the extraocular cơ do not allow efficient conjugate eye movements, which normally maintain corresponding thị lực objects on the retinas of both eyes Ballet’s sign Restriction of one or more extraocular cơ Lymphocytic invasion, viêm and phù dẫn đến xơ and scarring of the mắt cơ. Restriction of the range of movement then occurs Chemosis Swelling or phù of the conjunctiva tĩnh mạch compression and decreased tĩnh mạch drainage are likely to contribute. viêm tế bào infiltrate có thể also play a role Chemosis is also seen in reactions to allergies and foreign bodies Gaze limitation The bình thường range or field of vision is decreased viêm, swelling and cuối cùng xơ restrict the range of movement and contraction of the extraocular cơ. The eyeball cannot move as much and, do đó, vision becomes limited Sight loss Decreased vision tiến triển swelling of surrounding mô raises the orbital bony khoang pressure to a point at which the thị giác dây thần kinh is compressed andor damaged and vision is impaired or lost Periorbital fullness Swelling around the orbit chủ yếu do decreased tĩnh mạch drainage because of tĩnh mạch compression in the orbital space, leading to swelling of veins and capillaries and oedema49 lồi mắt (lồi mắt) Forward displacement of the eyes Swelling of the mắt cơ, fat pads and mô within the bony khoang ‘pushes’ the eyeball forward Riesman’s sign Bruit heard hơn the closed eye with a stethoscope Increased máu flow through the orbit gây ra bởi hyperdynamic state
Ý nghĩa lâm sàng: đái tháo đường retinopathy is an important sign and phải be monitored. The greater the extent of retinopathy at chẩn đoán, the higher the nguy cơ of tiến triển; this reinforces the importance of tight máu glucose control in a person with the Galactorrhoea in any man, and in a non-breastfeeding woman, warrants some attention. It is a non-specific sign that, if present, requires a thorough history and thăm khám in an attempt to find more localising signs. Some key facts to remember: • Galactorrhoea will occur in a majority of women with prolactinomas but is much Ít gặp in males.2 • 13% of bệnh nhân with to đầu chi có thể display galactorrhoea2 and 10% of bệnh nhân with nguyên phát suy giáp will have high levels of prolactin.35 • dưới 10% of cases of galactorrhoea are gây ra bởi systemic bệnh;36 thuốc-induced, vô căn, sinh lý and tân sản (e.g. prolactinoma) causes are Thường gặp. Goitre 523 Goitre Goitre (regardless of loại) is found in 70–93%41–43 of bệnh nhân with cường giáp. It do đó has relatively good sensitivity. tuy nhiên, lên đến 30% of elderly bệnh nhân have been found to have goitre without underlying tuyến giáp bệnh so it is less valuable as a specific sign10 for hormonal disturbance. A goitre with a focal nodule in the tuyến giáp nên luôn be investigated to exclude tuyến giáp cancer, đặc biệt in the setting of a euthyroid state. Goitre 524 Bảng 7.4 cơ chế of goitre development Hyperthyroid goitres Limited evidence exists on the true value of the sign. Historically, granuloma annulare has been liên quan đến loại 1 đái tháo đường and the degree to which it is related reviewed multiple times, without a definite link being found. Some of the evidence regarding this is as follows: • Cases have been reported with loại 2 DM.46 • It hiếm khi pre-dates the development of đái tháo đường.46 • In one study of 100 bệnh nhân with granuloma annulare, 21% of bệnh nhân with the generalised bệnh had đái tháo đường.47 • tuy nhiên. another study found a higher tỷ lệ mới mắc of đái tháo đường in localised granuloma.48 Graves’ ophthalmopathy (orbitopathy) 526 Graves’ ophthalmopathy (orbitopathy) Bảng 7.5 Classification of eye changes seen in Graves’ bệnh Class Definition No signs or triệu chứng Only signs (e.g. lid lag, upper lid retraction, stare) Soft mô involvement: periorbital phù, congestionredness of the conjunctiva, chemosis lồi mắt Extraocular involvement: upward gaze limitation, lateral gaze limitation Corneal involvement: keratitis Sight loss: thị giác dây thần kinh involvement Based on Werner SC, J Clin Endocrinol Metab 1969; 29: 782 and 1977; 44: 203; with permission. Graves’ orbitopathy or ophthalmopathy is thường gặp. khoảng 35–50% of bệnh nhân with Graves’ bệnh suffer from one or more đặc điểm,49,51 3–5% of bệnh nhân suffer from nặng eye bệnh,52 and lên đến 70% of bệnh nhân have subclinical eye bệnh identified on imaging. Many of the signs are very specific for underlying Graves’ bệnh. Quantifying the value of each individual sign is difficult; tuy nhiên, there is some evidence for the sau: • Lid retraction has a sensitivity of 34% and specificity of 99% and LR of 31.5 for Graves’ bệnh.41 • Lid lag has a sensitivity of 19% and specificity of 99% and LR of 17.6 for Graves’ bệnh.41 Graves’ ophthalmopathy (orbitopathy) 528 Bảng 7.6 Summary of eye signs in thyrotoxicosis and cơ chế Name